Alopecia: Understanding Different Forms of Hair Loss
Alopecia is the formal medical designation for any partial or complete loss of hair from the scalp or other body regions where hair normally grows. Hair loss affects an estimated 80 million people in the United States alone, making it one of the most common reasons patients seek dermatological evaluation. 1 Because alopecia functions as an umbrella term covering conditions with fundamentally different causes, mechanisms, and prognoses, accurately identifying the specific subtype is the essential first step before any management pathway can be considered.
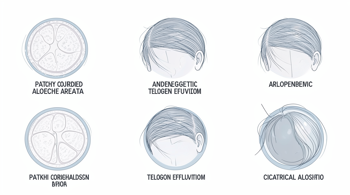
The Core Classification: Scarring Versus Non-Scarring Alopecia
Clinically, all forms of alopecia divide into two primary categories based on the structural fate of the hair follicle. Non-scarring alopecia is the most prevalent category; the follicle structure remains intact, meaning hair loss may be temporary and regrowth is biologically possible if the underlying cause is addressed. 2 Scarring alopecia, also called cicatricial alopecia, involves irreversible follicular destruction and replacement with scar tissue, making regrowth in affected zones permanently impossible. 3
This distinction carries direct clinical consequences. In non-scarring conditions, the therapeutic window is broader because viable follicles can still respond to intervention. In scarring forms, the priority shifts toward halting active inflammation and preserving surviving follicles rather than restoring lost ones. Early specialist evaluation is therefore particularly critical when scarring alopecia is suspected, since each week of delayed treatment can mean additional permanent follicular loss. 4
Androgenetic Alopecia: The Most Prevalent Subtype
Androgenetic alopecia, commonly described as male-pattern or female-pattern hair loss, is by far the most frequent form worldwide. It affects approximately 50 percent of men by age 50 and up to 40 percent of women by age 70. 1 Some lifetime prevalence estimates reach as high as 80 percent in men by age 70 and 50 percent in women over a lifetime. 5 The condition is driven by genetic sensitivity to dihydrotestosterone (DHT), a testosterone metabolite produced via the enzyme 5-alpha reductase. DHT binds to follicle receptors and progressively shortens the growth cycle, causing follicular miniaturization until the follicle ceases producing visible hair. 6
In men, the pattern typically presents as a receding frontal hairline and thinning at the crown, progressing along the Norwood scale. In women, the manifestation is usually diffuse thinning across the top of the scalp with a widening central part, assessed via the Ludwig scale. 7 Research suggests that topical minoxidil and oral finasteride can slow progression, though individual responses vary and benefits cease once treatment is discontinued, making these ongoing management tools rather than curative solutions. Minoxidil has demonstrated the ability to spur regrowth in approximately 40 to 60 percent of users within roughly six months of consistent use. 5
Alopecia Areata: The Autoimmune Dimension
Alopecia areata is an autoimmune disease in which the immune system mistakenly targets hair follicles, producing sudden, well-defined patchy hair loss on the scalp, face, or body. Nearly 7 million people in the United States currently have some form of alopecia areata, and the condition carries an estimated lifetime prevalence of approximately 2 percent globally. 8 Because the follicle itself is not permanently destroyed in most cases, spontaneous regrowth can occur, though relapse is common and the clinical course is highly unpredictable.
The condition exists on a spectrum of severity. Alopecia totalis refers to complete scalp hair loss, while alopecia universalis denotes the complete loss of all scalp, facial, and body hair. 9 Nail changes, including pitting and brittleness, can accompany the hair loss and serve as a diagnostic indicator. Treatment approaches have historically included corticosteroid injections and topical immunotherapy, while more recent advances involve JAK-STAT inhibitors, a class of targeted therapies that address the underlying immune signaling pathways driving follicular attack. 10
Telogen Effluvium and Anagen Effluvium: Stress and Toxin-Driven Shedding
Telogen effluvium is the second most common form of hair loss and is characterized by diffuse, excessive shedding triggered when a physiological or psychological stressor pushes a disproportionately large number of follicles simultaneously into the resting (telogen) phase. Common triggers include major surgery, high fever, significant weight loss, childbirth, iron deficiency, and severe emotional stress. 11 Because shedding typically begins two to four months after the triggering event, patients often struggle to connect cause and effect. The condition is generally self-limiting and resolves within six to nine months once the trigger is identified and corrected. Ensuring adequate intake of iron, zinc, and biotin may support healthy regrowth during recovery. 6
Anagen effluvium is a distinct form of hair loss occurring during the active growth phase rather than the resting phase. It is most frequently associated with chemotherapy or radiation treatments, which disrupt rapidly dividing cells including those in hair follicles. Unlike telogen effluvium, anagen effluvium can produce sudden, widespread hair loss across the scalp and body within weeks. 2 In the majority of cases, regrowth resumes after the causative treatment ends, though hair texture and color may temporarily differ during the recovery period.
Traction Alopecia and Scarring Alopecia: Mechanical and Inflammatory Origins
Traction alopecia results from sustained mechanical stress on hair follicles caused by tight hairstyles such as braids, buns, extensions, or cornrows. The repeated pulling gradually damages follicle architecture, initially producing a non-scarring pattern of hair loss along the hairline and temples. 12 If the mechanical tension persists over an extended period, permanent follicular damage and scarring can develop, transitioning what was a reversible condition into an irreversible one. Early recognition and modification of hairstyling practices are therefore the primary intervention strategy.
Scarring alopecias as a broader group include conditions such as lichen planopilaris, frontal fibrosing alopecia, discoid lupus erythematosus, and central centrifugal cicatricial alopecia. All share the feature of progressive inflammatory destruction of follicles with permanent replacement by fibrous tissue. 3 Scalp biopsy is frequently required to confirm the diagnosis and identify the specific subtype, since treatment regimens differ considerably across scarring conditions. Fungal infections such as tinea capitis can also produce inflamed, scaly scalp patches and hair loss, but require antifungal therapy rather than standard alopecia treatments. 13
Diagnosis, Psychological Impact, and Key Considerations
Accurate diagnosis of alopecia relies on a combination of clinical examination, patient history, dermoscopy, blood tests to identify underlying deficiencies or hormonal imbalances, and scalp biopsy when scarring or ambiguous presentations are involved. 2 The psychological burden across all subtypes is well-documented. Both male and female pattern baldness are associated with low self-esteem, depression, and social isolation, with women reporting greater emotional impact on average. Research further indicates that androgenetic alopecia has been associated with increased rates of anxiety and depression, reinforcing that hair loss is not merely a cosmetic concern. 14
| Type | Primary Cause | Reversibility | Key Feature |
|---|---|---|---|
| Androgenetic Alopecia | Genetic / DHT sensitivity | Partially manageable | Patterned thinning by scale |
| Alopecia Areata | Autoimmune | Possible but unpredictable | Patchy, sudden onset |
| Telogen Effluvium | Physiological stressor | Usually self-limiting | Diffuse shedding, delayed |
| Anagen Effluvium | Chemotherapy / radiation | Generally reversible post-treatment | Rapid, widespread loss |
| Traction Alopecia | Mechanical tension | Reversible if caught early | Hairline and temple recession |
| Scarring Alopecia | Inflammatory / fibrotic | Permanent in affected zones | Follicle destruction, requires biopsy |
Support organizations such as the National Alopecia Areata Foundation (NAAF) and the Scarring Alopecia Foundation (SAF) provide patient resources and connect individuals with clinical research opportunities. Dermatologists, and in complex cases dermatopathologists, remain the appropriate specialists for evaluation, since the wide variation in alopecia subtypes means that treatment strategies effective for one form may be entirely inappropriate or counterproductive for another. 8
Sources
- National Dermatology Authority - nationaldermatologyauthority.com
- Penn Medicine - pennmedicine.org
- Cleveland Clinic via DermCare Experts - dermcare.expert
- Acibadem International Hospitals Group - acibademinternational.com
- HealthVetted - healthvetted.com
- HairCited - haircited.com
- ALMO Clinic - almoclinic.com
- WebMD Health Discovered Podcast - webmd.com
- New England Associates - newenglandassociates.com
- IJPS Journal - ijpsjournal.com
- Canadian Dermatology Association - dermatology.ca
- American Academy of Dermatology via Advanced Hair - advancedhair.com
- Centers for Disease Control and Prevention - cdc.gov
- Acorn Biolabs - acorn.me
Authored by MyTrendSpot team